Low back pain may be the most common diagnosis seen in doctor and physical therapy clinics. How about this for statistics from an article published by the American Academy of Family Physicians:
Low back pain may be the most common diagnosis seen in doctor and physical therapy clinics. How about this for statistics from an article published by the American Academy of Family Physicians:
- Low back pain is the 5th most common reason for all physician visits.
- Low back pain is responsible for more than $20 billion annually in direct health care costs.
- In the United States, approximately 90% of adults experience back pain at some time in life.
- 100% of people writing this post (OK, me…) are currently experiencing low back pain. Seriously, I have had a bad few days…
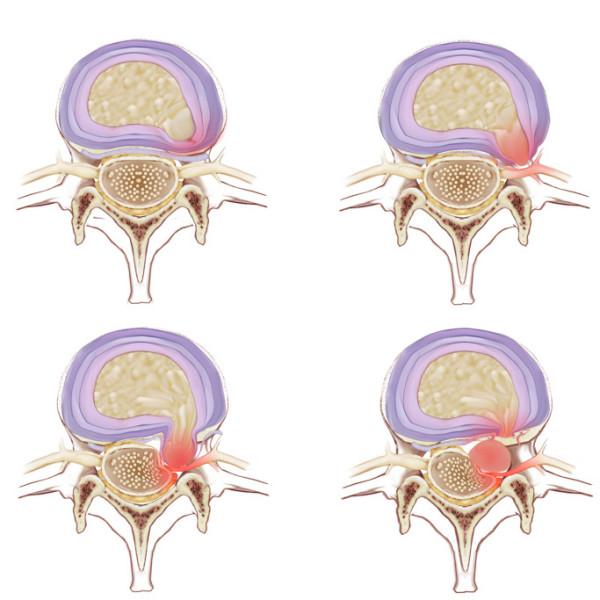
This is why I found an new research report published in the Journal of Orthopedic Surgery and Research on the accuracy of MRI in detecting lumbar disc herniation. Surprisingly, there are few articles in the literature o the accuracy of MRI for patients with low back pain. The authors prospectively evaluated the MRI’s of 50 patients undergoing open lumbar microdiscectomy.
They found MRI to be 72% sensitive, 68% specific, and 70% accurate in detecting containment status of lumbar herniated discs. More specifically 28% of patients that showed a disc herniation on MRI actually did NOT have one during surgery. Conversely, 33% of patients with a negative MRI actually had a herniation.
Clinical Implications
I must admit that these results are surprising for me. Maybe this is why there appears to be such a high volume of asymptomatic people with lumbar disc herniations. I never think that MRI’s are perfect but being wrong 30% of the time seems high to me when the results have a significant impact on surgical decision making. Luckily low back pain tends to respond well to conservative treatment. This study only further supports the use of physical therapy in an attempt to treat low back pain nonoperatively.
This study also stresses the point that we should never treat a MRI and should always base treatment on the patient’s symptoms and the results of a thorough examination. Here are a couple more free online articles on the topic that I have found:
- Clinical evaluation and treatment options for herniated lumbar disc
- Diagnosis and management of acute low back pain
A question for those readers who are trained in a certain diagnostic method (i.e Maitland, McKenzie, etc, or even better, more than one type of training) – do you feel that a specific approach has been more accurate in diagnosing disc herniations that will not respond to conservative treatment? What has been your experience?
Bradley K Weiner, Rikin Patel (2008). The accuracy of MRI in the detection of Lumbar Disc Containment Journal of Orthopaedic Surgery and Research, 3 (1) DOI: 10.1186/1749-799X-3-46