
 Glenohumeral internal rotation deficit, or GIRD, continues to be one of the most polarizing topics in baseball sports medicine. It has become so popular that even athletes and the general public know about GIRD, often exhibiting fear and anxiety with just the mention of GIRD.
Glenohumeral internal rotation deficit, or GIRD, continues to be one of the most polarizing topics in baseball sports medicine. It has become so popular that even athletes and the general public know about GIRD, often exhibiting fear and anxiety with just the mention of GIRD.
How many times has a baseball player come back from the doctor with their head down saying, “I have GIRD,” as if the world has just ended?
I do not feel that everyone truly understands GIRD, how to assess GIRD, or how to treat GIRD. There are a lot of theories and assumptions out there that may or may not be true.
Here is my take on GIRD, and it is not exactly how everyone would describe GIRD.
What is normal range of motion in an overhead athlete?
Before we can have any discussion on what is considered abnormal range of motion in the thrower’s shoulder, we should make sure we understand what is considered “normal” in overhead athletes.
Throwers have very unique adaptations from the demands of throwing. Numerous articles over the past 15 years have consistently shown that the dominant shoulder in overhead athletes exhibits an increase of external rotation and a subsequent decrease in internal rotation. However, if you take the total rotation motion and combine ER and IR measurements the numbers are almost identical.
I remember when we first started discovering this phenomenon many years ago and it is uncanny how you find essentially the exact same total motion arc on both sides.
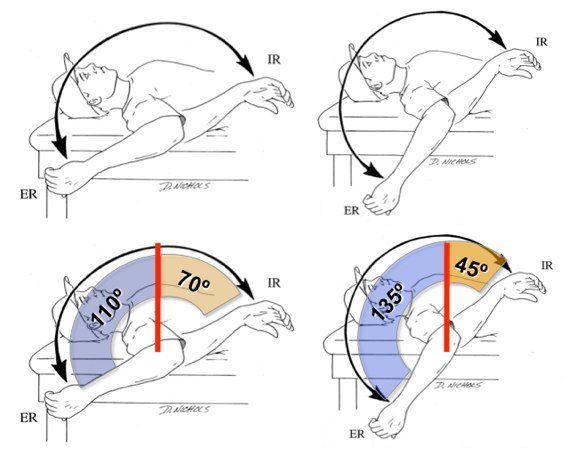
Here is an illustration of what this looks like. In this figure. You see the nondominant shoulder on the left and the dominant shoulder on the right. You see the shift in the arc of total rotational motion, however if you break down the components of ER and IR, you see that both sides total 180 degrees.
This adaptation has been shown in too many publications to list here, but I’ll add a few:
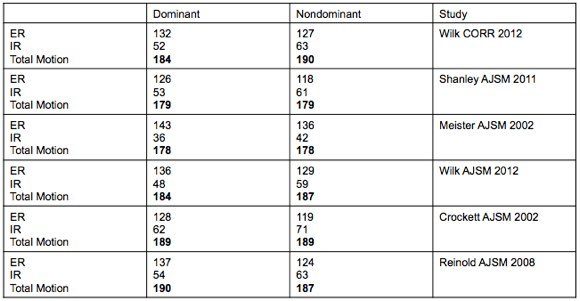
This is a brief list but you can see that the total rotation motion on both the dominant and nondominant shoulders is almost identical in every study. Statistical analysis revealed no significant differences in range of motion side to side.
Why the Adaptation in Shoulder Range of Motion?
Since the first discovery of this loss of internal rotation on the throwing arm, there have been several theories as to the specific reason for the adaptation.
The first theory centered around the fact that since there was a loss of internal rotation, there must be a subsequent tightness of the posterior capsule. In actuality, this is really a long shot of being the isolated reason for the loss of IR, assuming a very specific cause for GIRD.
With so many potential factors contributing to the altered range of motion, it is surprising to me how popular this theory became. If IR is less on the thrower shoulder, we now jump straight to recommending aggressive internal rotation and posterior capsular stretching. I guess whatever theory comes out first gets the most traction and popularity!
The major flaw of the posterior capsule tightness theory is that it does not take into consideration the very specific increase in ER that is also seen in overhead athletes, let alone the fact that total rotational motion is still the same side-to-side. If the posterior capsule was the cause of the loss of IR, would we then assume that the anterior capsule has loosened precisely the exact same amount to allow the exact same increase in ER as the posterior capsule does to restrict IR?
That sounds pretty unrealistic to me.
Shortly after the posterior capsule tightness theory was presented, many researchers took a more scientific look at what could be causing this very precise shift in the arc of motion in baseball pitchers and other overhead athletes. Several studies have now been published that have assessed boney changes that could be associated with GIRD. Using both MRI and CT scans, it is now well documented that the humerus of the throwing arm is more retroverted than the nondominant arm.
What this means is that the actual bone of your upper arm torques and adapts.
Imagine twisting and wringing out a towel. This is exactly what happens to the humerus during throwing while your growth plates are open. The body, bones especially, do a great job of adapting to stress. Essentially, the humerus bone of your upper arm twists at the growth plate and causes permanent adaptations to your bones. Newer research is also now showing that the other end of the socket, the glenoid, also shows retroversion.
Based on these studies, the exact amount of retroversion observed appears to be approximately 10 degrees on average. Now go back up and look at the table above. Notice how the loss of IR is approximately 10 degrees and the gain of ER is approximately 10 degrees? This boney adaptation makes the very specific shift in range of motion make more sense. I have shown a simple and fairly effective way of measuring humeral retroversion in the clinic. Try it in your throwers and you’ll see.
Pretty cool, right? Still think the posterior capsule is the cause of loss of IR?
I was also a part of two studies that looked at glenohumeral translation in the baseball pitcher that both showed that posterior translation was twice that of anterior translation. This was even present in baseball pitchers with as little as 10 degrees of IR. They still had a large amount of posterior translation, not posterior capsular tightness.
Taking all of this into consideration, if there is one thing you take away from this article, it should be:
[quote]The thrower’s shoulder is supposed to have less IR on the dominant side. This is normal.[/quote]
Determining What is Clinically Significant GIRD
A threshold to determine what can be considered a clinically significant loss of IR is vitally important to the implementation of programs designed to prevent and treat GIRD. As previously discussed, a loss of IR itself can be considered a normal anatomical variation observed in overhead athletes.
Despite this finding, the term GIRD has continued to have a negative connotation, implying that any side-to-side loss of IR may be pathological. This has resulted in a trend towards assuming many of the hypothesized theories of why loss of IR occurs are present in each person.
This unfortunately leads to a standardized prescription of stretches and exercises based on assumption and not a thorough assessment.
After reviewing the literature, it appears that most authors have been arbitrarily defining GIRD as a loss of IR greater than 15-20 degrees in comparison to the nonthrowing arm. Some authors have even published studies showing that your chance of getting injured is increased if you have GIRD of more than 15-20 degrees.
Correlating GIRD to injury is too simplistic at best and again has too many flaws to consider this valid.
You can not accurately state why an increase in injury was observed. Was it the loss of 17 degrees of IR? Or perhaps the subsequent gain of 17 degrees of ER? You can’t make a definitive conclusion either way.
[quote]Perhaps the increase of injuries in baseball pitchers is due to the gain in shoulder ER, not GIRD and the loss of IR?[/quote]
I am thinking this more and more everyday.
Another major flaw with defining GIRD using an arbitrary number is that the published amounts of range of motion have a very large standard deviation. If you look through the published studies on GIRD, you’ll see that the standard deviation of measurements is large, ranging from 8 degrees to over 15 degrees. That means the “normal” amount of internal rotation on a shoulder is approximately 50 degrees, but plus or minus 15 degrees. Thus both 35 degrees and 65 degrees of internal rotation should be considered “normal.”
I can say that I have observed this first hand in professional baseball pitchers. I have seen just as many players with 140 degrees of total rotational motion than I have with 200 degrees of total rotational motion. Sure, this averages out to 170 degrees. But not all baseball pitchers have 170 degrees of total rotational motion.
With such a large standard deviation and variability in measurements, assigning an arbitrary number to define GIRD is too simplistic.
A New Definition of GIRD
These findings have caused me to alter the way I define GIRD and stimulated me to propose a new definition of GIRD based on total rotational motion.
Previous definitions of GIRD based on arbitrary numbers have resulted in generalized treatment programs that are not specific or individualized enough to be utilized in clinical practice.
I propose that a loss of side-to-side IR is actually a normal anatomical variation in overhead athletes and should not be considered pathological GIRD unless there is a subsequent loss of total rotational motion in the dominant arm as well.
This definition essentially takes the large variability in ROM that has been observed in athletes into consideration and allows for a more individualized approach to treating GIRD. So:
[quote]GIRD is a loss of internal rotation range of motion in the presence of a loss of total rotational motion.[/quote]
In this new definition of GIRD, a pathological condition of GIRD is defined as a loss of IR in the presence of loss of total rotational motion.
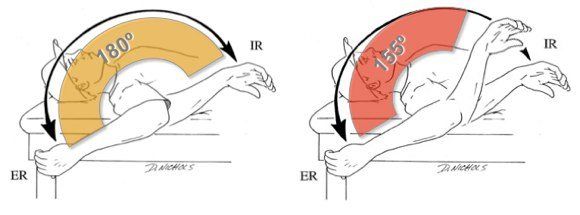
Lets looks at this as both an illustration and an equation. In the figure below, you see the normal arc of motion in an overhead athlete, and to the right, an altered total rotational range of motion due to a loss of IR.
You can observe this yourself by assessing the specific range of motion measurements. To calculate GIRD, use this equation:
GIRD = (Side-to-side difference in ER) + (Side-to-side difference in IR)
Here is an example of two baseball pitchers with a loss of IR:
- Player 1 = (D ER 120 deg – ND ER 100 deg = +20 deg ER) + (D IR 60 deg – ND IR 80 deg = -20 deg IR) = 0 deg – Despite a loss of 20 degrees this is not pathological GIRD because total motion is the same bilaterally
- Player 2 = (D ER 120 deg – ND ER 100 deg = +20 deg ER) + (D IR 35 deg – ND IR 80 deg = -45 deg IR) = -25 deg GIRD – This represents a pathological GIRD because both IR and total rotational motion are limited
I would suggest that the first player above should not be considered or even called GIRD, despite the fact that there is 20 degrees less IR on the throwing shoulder. Because the total motion is the same, this is a normal adaptation in this athlete.
In fact, I would comfortably say in my experience that if you tried to reduce that 20 degrees loss of IR when total motion is symmetrical, you would essentially be increasing the total rotation motion and creating instability in an already vulnerable joint.
I believe this causes more injuries than it helps.
Because of the negative association that we have established with the word GIRD, I would propose that we stop calling everything GIRD and reserve GIRD for when it is truly pathological. This helps clear up confusion.
I strongly feel that this new definition of GIRD takes the individual variability of range of motion as well as the total rotation motion into consideration and is a much more accurate calculation to base treatment recommendations.
Why is this important?
The goal of this article is to share my experience treating baseball pitchers. I have rehabilitated 1000’s of injured baseball pitchers and managed 1000’s of healthy baseball pitchers. This unique experience really opened my eyes to what is “normal” in baseball players.
When I first started working in Major League Baseball, I quickly found out that much of what I believe to be “facts” were not always accurate. I’ll be the first to admit this. If you only treat injured baseball pitchers, you start to assume that some normal adaptations may be pathological.
While my experience has been with baseball pitchers, this information can be extrapolated to all overhead athletes as these findings have all been established in other sports, such as tennis and handball.
There are far too many people who see a loss of IR and immediately label it GIRD. Furthermore, there are far too many people who label any loss of IR as GIRD and blindly treat the posterior capsule. I’m not saying that posterior capsular tightness does not exist, I am just saying it exists far less than we are diagnosing it and there are many other reasons that we need to consider before we start challenging the integrity of the stabilizing structures of the thrower’s shoulder. I even dedicated an entire webinar to showing you 5 ways to gain IR without stretching the posterior capsule.
Blindly assuming GIRD is pathological, stretching the heck out of IR, and treating the posterior capsule is harmful.
Assess, Don’t Assume
Even with a pathological GIRD using the above equation, you can not assume you know why they have a loss of IR.
I have previously published a study showing that there is an immediate loss of IR after pitching. We theorized that this was too acute to represent any changes in the capsule and most likely represented muscular stiffness from the eccentric trauma associated with pitching. This was even more apparent when we also noticed that there was a loss of elbow extension, which is also subject to extreme eccentric forces during throwing.
You can’t assume they need to be stretched to gain more IR or that the posterior capsule is tight. Maybe it is. Maybe it isn’t. Regardless:
Assess, don’t assume.
There is a specific way to assess the posterior capsule, which I will share in an upcoming post. In fact I am going to write a series on how to more accurately assess GIRD, internal rotation, and the posterior capsule.
By changing the way we assess and define GIRD, we can start to more accurately understand what is happening to these overhead athletes and provide the best care possible.



